PARAPHILIC DISORDERS
Fetishistic Disorder: When a Fetish Causes Distress
Fetishes can be quite common among most people, even if it’s not an openly discussed subject. Nevertheless, there have been attempts to start conversations about it. This can be observed from the multitude of articles from lifestyle magazines that attempt to normalize common fetishes or organizations that aim to improve sexual health literacy/sex education. However, what is still relatively undiscussed is fetishistic disorder – what is it exactly?
What is a Fetish - Fetishism versus Fetishistic Disorder
While both involve experiencing sexual arousal from non-living object(s) or non-genital body part(s), fetishistic disorder results in significant distress or impairment in life/functioning. Impairment can manifest itself in various ways. Sexual dysfunction might occur in romantic relationships – some individuals might not be receptive to their partner’s fetish. There are also instances where individuals with fetishistic disorder may prefer solitary sexual activity associated with their fetishistic preference(s) even if they are currently in a happy and fulfilling relationship. Therefore, some individuals might not engage in proper sexual activities with their partners, potentially resulting in marital issues. Some individuals also go on to commit crimes that are primarily motivated by their fetish(es), such as theft/burglary or taking upskirt photos (in cases where the individual has an underwear fetish or voyeuristic-disorder).
What is Fetishistic Disorder?
According to the Diagnostic and Statistical Manual of Mental Disorders, 5th edition, a diagnosis of fetishistic disorder is given if the following criteria are met:
Over a period of at least 6 months, recurrent and intense sexual arousal from either the use of non-living objects or a highly specific focus on non-genital body part(s), as manifested by fantasies, urges or behaviors.
The fantasies, sexual urges or behaviors cause clinically significant distress or impairment in social, occupational or other important areas of functioning
The fetish objects are not limited to articles of clothing used in cross-dressing (as in transvestic disorder) or devices specifically designed for the purpose of tactile genital stimulation (e.g vibrator).
The DSM-5 also classifies fetishistic disorder into several subtypes, depending on what the individual’s fetish is (body part(s), non-living object(s), others). It also specifies if an individual is currently in a controlled environment or in full remission.
Onset and Comorbidities
Fetishistic disorder typically has its onset in puberty, though fetishes can develop prior to adolescence. Once established, fetishistic disorder tends to have a continuous course that fluctuates in intensity and frequency.
Fetishistic disorder might occur commonly with other paraphilic disorders, such as voyeuristic and/or transvestic disorder. In some instances, clients might also feel guilty about their behavior and experience depressive moods and anxiety as a result. Fetishistic disorder might be associated with neurological conditions too, though this is rare.
Addressing Fetishistic Disorder
People with fetishistic disorder do not seek help often – this can be attributed to a few reasons. One reason could be that they do not find their behavior problematic until they run into trouble with the law. Another reason could be that while they feel their preferences are uncommon/unusual, as sex is a taboo subject, they are reluctant to seek help for it or shame prevents them from doing so. Nevertheless, there are instances where individuals with fetishistic disorder seek help as they experience significant distress. In such instances, it’s recommended that medication and therapy are used in tandem to address fetishistic disorder. Here are some therapy modalities that can be utilized.
Psychoeducation will be provided to the individual via two ways – by using the offence cycle (as illustrated in the picture below) and the Good Lives Model. The clinician will make use of a framework (offence cycle) to improve the individual’s awareness of their internal states that increase the probability of offending. Here is an example of the framework:
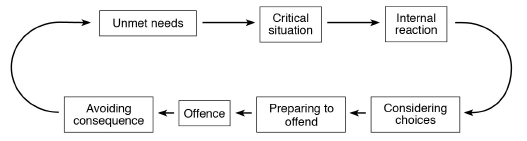
Credits: Clinical Psychology in Singapore: An Asian Casebook
The Good Lives Model is aimed at motivating the individual, such that they are less inclined to reoffend. This is done via a strengths-based rehabilitation approach, with the clinician and client working together to develop and implement meaningful life plans that are incompatible with the offending behaviors.
Cognitive-behavioral therapy (CBT) is a viable option in managing the psychopathology of fetishistic disorder, where the clinician would work with the individual to identify the underlying cause of their behavior and teach them ways on managing sexual urges in healthier and more adaptive ways. Certain techniques will be utilized during therapy, such as cognitive restructuring and covert sensitization. Cognitive restructuring is aimed at guiding the individual in identifying and changing thoughts that cause the behavior. Covert sensitization, on the other hand, is aimed at increasing the salience of negative consequences of deviant sexual behavior to the individual. This is done by getting the client to visualize deviant sexual behavior and the negative events/consequences that follow (e.g being arrested). Following this, the clinician then works with the individual to produce a non-offending script – the client is asked to visualize deviant behavior and ways they can prevent negative consequences/events from occurring. This will act as a model for prosocial behavior, where the association between deviant behavior and preventive measures becomes stronger over time, hence reducing the likelihood of an individual committing such acts.
In some instances, medication is prescribed to reduce an individual’s preoccupation with the sexualized object and sexual arousal. This includes anti-depressants like SSRIs. It also includes anti-androgens (testosterone-lowering drugs) aimed at lowering the potential for sexual arousal, or the potential for sexual performance in response to sexual arousal. Some forms of medication may also reduce compulsive thinking associated with fetishistic disorder, hence improving an individual’s ability to focus during therapy.
Prognosis
The prognosis of fetishistic disorder can be rather limited, given that it is a chronic condition with its onset in adolescence. Among those who attend therapy, approximately half may relapse. In addition, as some individuals do not see it as a problem, they may choose to terminate therapy prematurely, hence increasing the probability of relapses.
Nevertheless, it is possible to manage fetishistic disorder after one spends some time in therapy. It is recommended that therapy is conducted long-term, given that fetishistic disorder tends to fluctuate in intensity and frequency of urges or behavior over the course of an individual’s life. The success of therapy is dependent on the individual’s motivation level during therapy. Some might be motivated by the fear of being arrested or incarcerated. In addition, some individuals might persevere with therapy as they find that it plays an important role in mending the relationship between them and their loved ones, or that they do not wish for their family members to continue experiencing shame for their condition.